
Need to know

For #TeamEEAST Last updated: 19 April 2024 at 06:32

Here’s a quick refresher from the clinical team on managing patients suffering a STEMI with right ventricular involvement (RVI)…
Statistics:
Diagnosis:
Standard 12-lead with inferior STEMI and RVI
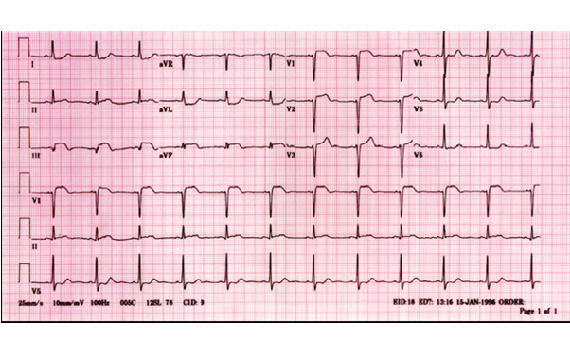
Note the ST elevation in V1-V3, and the maximal ST elevation in lead three. This is a typical pattern of an inferior STEMI with RV involvement.
Same patient with right sided V leads
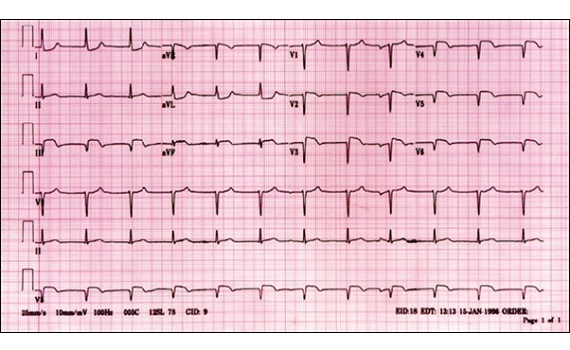
In this ECG, all V leads are placed across the right side of the chest. Please note maximal ST elevation in RV4. It’s recommended to only place V4 in the right-sided position pre-hospitally.
Treatment
Nitroglycerin is generally indicated in myocardial infarction because of the drug’s vasodilatory effects on blood vessels. This could lead to decreased ischemia, decreased myocardial oxygen consumption and subsequently, an improvement in blood flow to the myocardium.
However, vasodilators, diuretics, and morphine are not well tolerated by patients with RVI and may lead to severe hypotension. The effects of these medications may cause a reduction in preload by decreasing filling pressures and subsequently decreasing cardiac output.
Therefore volume loading with a sodium chloride solution is recommended as the initial therapy in RVI. Progressive volume loading can produce an incremental increase in right-sided filling pressures, systolic blood pressure and cardiac output. Fluid volume loading is based on Starling’s law, which states that the greater the amount of stretch of the ventricle, the more forceful the contraction.
Published 21st December, 2015