
Need to know

For #TeamEEAST Last updated: 25 April 2024 at 13:13

A few weeks ago we published an article about mandatory capnography, and a few of you got in touch to say that you weren’t sure how to grade the view of the cords in intubation.
So we asked Chris, the Trust’s Trauma Lead, to write a short refresher guide for you.
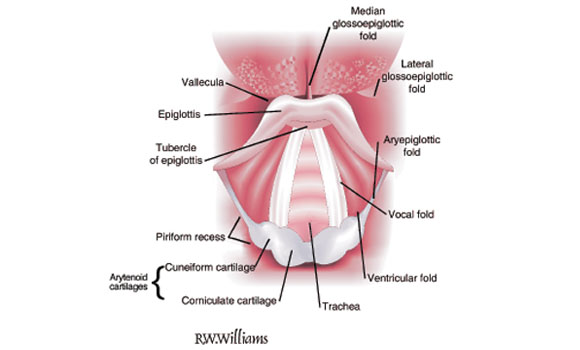
Firstly, it’s important to know your airway landmarks in order to best appreciate and appropriately report on the grading of cords.
Key aspects that will be crucial in assessing grading view:
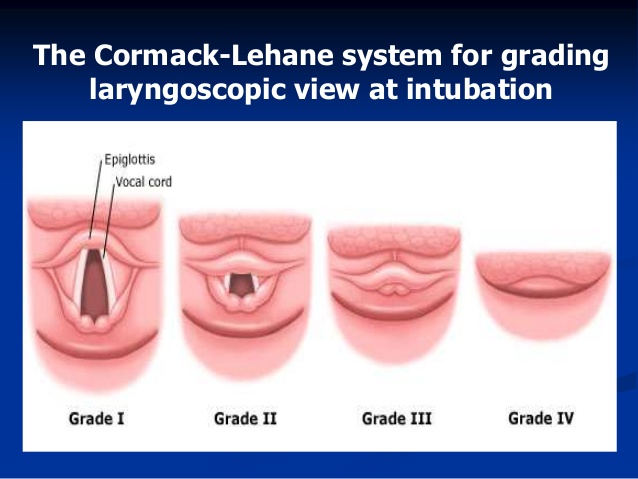
The grading system used is called the Cormack-Lehane system, and it applies a grade of 1 to 4 (reported as I, II, III, IV) depending on what anatomy is visible whilst performing laryngoscopy.
As much as LEMON (and specifically the Mallampati aspect) can be used as a predictor, it is not until direct laryngoscopy is undertaken that you’ll know what grade view you are presented with.
Remember good laryngoscopy techniques to perform the procedure:
Grade I
All identifiable anatomy will be visible including all of the vocal cords, a wide tracheal opening and the aryepliglotic folds making up the sides of the tracheal opening. Note - even with a grade I view, a bougie must be used to pass the endotracheal tube (ETT) to ensure a first-time pass.
Grade II
In this view there will still be direct sight of a tracheal opening and a view of the base of the vocal cords, but you won’t be able to see the side walls (aryepiglotic fold). At this stage the arytenoid cartlages become one of the prominent features of land marking.
Grade III
The arytenoid cartilages, along with the epiglottis, become the only identifiable landmarks for knowing where the tracheal opening will be. A complete loss of tracheal opening and vocal cords make a grade III view. At this stage, intubation becomes very difficult and any attempt at passing an ETT must be with the use of a bougie and will probably necessitate the use of a stylet to shape and guide the tube. ETCO2 now becomes the saving grace for confirming placement.
Grade IV
A complete loss of ALL landmarking features, including valeculla and epiglottis. Needless to say this view is commonly associated with failed intubations as there is a complete lack of guiding features to know where the trachea is. Any intubation attempts would need to be as a last resort, ideally attempted by skilled and advanced trained clinicians with kit suited to meet the needs of the situation. This is where your critical care paramedics and enhanced medical teams can assist.
Remember, providing your patient doesn’t have a spinal injury there are a few things you can do to maximise airway positioning and improve your view for intubation.
Tilt the head and life the chin, and put a blanket or mediwrap under the head to raise it off the ground. If your patient is bariatric, ramp their upper back and torso. Making sure your equipment is properly prepared will help you in making the first attempt the best attempt.
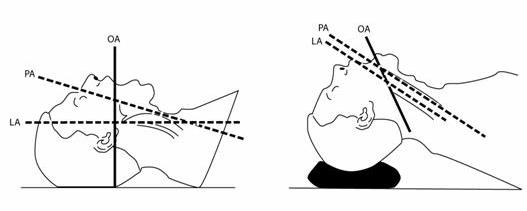
OA = Oral aspect, PA = Pharyngeal aspect, LA = Laryngeal aspect
Remember:
Published 13th August, 2015